
Shock is defined as an acute clinical syndrome characterized by hypo perfusion and severe dysfunction of vital organs.
Classification of Shock :
1. Hypovolemia shock
2. Cardiogenic shock
3. Distributive shock
4. Obstructive shock
1. Hypovolemia shock :
Causes :
1. Loss of extracellular fluid:
a. Deviation of normal exchange pattern: As in vomiting, diarrhea, intestinal obstruction, peritonitis, and acute pancreatitis.
b. Increased sweating without replacement in a non- acclimatized individual.
c. Third space shift to sodium from extracellular to intracellular compartment due to failure of sodium pump caused by hypoxia.
2. Plasma loss: due to burn.
3. Hemorrhage:
Due to whole blood loss like.
a. Surgical: During and following any major surgery especially cardiopulmonary bypass, pelvic surgery or major abdominal surgery.
b. Traumatic: As a result of any type of major accident, warfare injuries, homicidal or following suicidal injury as by knife, bullet, etc.
c. GI bleeding: Bleeding from peptic ulcer, perforation of intestine, bleeding from esophageal varices, etc.
d. Obstructive bleeding: Incomplete abortion, placenta previa, etc.
Clinical Features :
1. Anxiety, restless, excitation and disorientation.
2. Pallor
3. Thirst and hunger
4. Cold and clammy skin
5. Faint in upright position
6. Tachycardia with rapid, thready pulse.
7. Hypotension
8. Oligouria or anuria.
Management :
1. Control haemorrhage.
2. IV fluid is to restore circulating blood volume.
3. Blood transfusion.
4. Rising of foot end of bed.
5. Oxygen inhalation.
6. If acidosis develops. Sodium bicarbonate is infused till PH is normalized.
7. Recovery is indicated by improvement in consciousness, dry and warm skin, CVP is more then 5 cm of H₂O, distended veins and increased in urinary eoutput.
2. Cardiogenic shock :
-Myocardial infection is the most common cause of cardiogenic shock.
-Cardiogenic shock occurs if more then 40% of left ventricle is involved in acute infection.
-Elevated cardiac chamber filling procedure is hallmark of cardiogenic shock.
Clinical features of cardiogenic shock :
-The primary problem is decrease in contractility of heart, due to decrease contractility there is decrease in stroke volume.
-The patient present with tachycardia, low blood pressure and decrease urinary output.
-The jugular venous pressure may be raised.
-The peripheries are cold and patient may be confuse or “moribund.
Treatment :
-Oxygenation is improved by providing oxygen through facemask or endotracheal intubations.
-Ionotropes may improve cardiac contractility.
-Vasodilation such as nitroglycerine is adminis- tered to dilate coronary arteries and peripheral vessels to improve tissue perfusion.
-Intra-aortic balloon pump or ventricular assist devices are used to help ventricles.
3. Distributive shock :
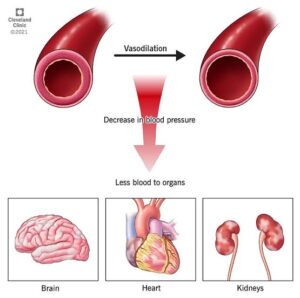
This occurs when the after load is excessively reduced. Distributive shock occurs in following situations:
a. Septic shock
b. Anaphylactic shock
c. Neurogenic shock
a. Septic shock :
– This type of shock is mostly due to release of endotoxins in blood, which causes wide spread vasodilation of blood vessels resulting in fall in the cardiac output. Fall in the cardiac output is not initial feature and vasoconstriction is not observed.
-Bacteria responsible for release of endotoxins are E. coli, Pseudomonas proteus, etc.
Clinical feature :
1. Restlessness, anxiety
2. Cyanosis
3. Cold and clammy skin
4. Tachycardia
5. Oligouria or anuria
6. Acidotic breathing.
Management :
1. Sedation with diazepam
2. I/V fluids.
3. Blood culture and sensitivity.
4. Antimicrobial agents: Combination of penicillin or cephalosporins and amino glycosides and metronidazole.
5. Injection hydrocortisone
b. Anaphylactic shock:
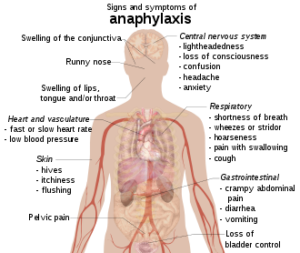
-This type of shock is a result of Type I hypersensitivity reaction.
-Anaphylactic shock can occur when a previously sensitized individual is exposed to a specific antigen, IV. Drug, specially penicillin, cephalosporins and iodinated contrast media are common offenders.
Clinical Features :
1. Due to reduced cerebral perfusion there is change in mental status.
2. Due to reduced preload and cardiac contractility there is hypotension.
3. Due to release of histamine and other chemical mediators there is urticaria.
4. Due to hypoxia the cyanosis is caused.
5. Due to anaerobic metabolism and hepatic dysfunction the lactic acidosis is caused.
6. Due to coronary ischaemia other dysrhythmias are caused.
c. Neurogenic shock:
-This is response to sudden fear or severe pain and the effects from slight fainting fit to death.
-This type of shock is also known as neurogenic or psychogenic shock.
-There is sudden pooling of blood in the capacitance vessels of legs and splanchnic arterial bed. This causes hypoxia of vital center.
Clinical Features :
– History of emotional stress or pain of a sudden nature.
– Bradycardia or pallor.
– Tachypenia
– Fainting
– Reflexes are usually intact.
Management :
– Place the patient flat or in head low position.
-Ensure potency of airway
-IV atropine may be needed for persistent or increasing bradycardia.
4. Obstructive shock :
-The obstructive shock is due to cardiac temponade, due to tension Pneumothorax and pulmonary embolus.
-In cardiac temponade there is compression of all chambers of heart with reduce cardiac output. The filling pressure of left and right-sided chambers equalizes. The central venous pressure is high and the BP is low.
Treatment :
-To maintain preload with fluid or blood.
– Relief of obstructions, drain pericardial cavity as early as possible.