
Most salivary gland tumors arise from the epithelium of the duct apparatus, but occasionally lesions seem to show acinar cell differentiation. Acinic cell carcinoma is a malignant epithelial neoplasm in which the neoplastic cells express acinar differentiation. Some authors advocate the existence of both benign and malignant acinic cell neoplasms, whereas others are of the opinion that all acinic cell neoplasms are malignant. Unfortunately, the criteria for distinguishing between benign and malig- nant acinar cell tumors, if such a distinction exists, have not been clearly established. In an extensive study of acinic cell tumors of the major salivary glands by Abrams and his coworkers, it was concluded that most investigators believe that all tumors of this type have at least a low-grade malignant potential. By conventional use, the term acinic cell carcinoma is defined by cytologic differentiation towards serous acinar cells (as opposed to mucous acinar cells), whose characteristic feature is cytoplasmic PAS-positive zymogen-type secretory granules.
In AFIP data of salivary gland neo- plasms, acinic cell carcinoma is the third most common malignant salivary gland epithelial neoplasm after mucoepidermoid carcinoma and adenocarcinoma. In this data, acinic cell carcinoma comprised 17 percent of primary malignant salivary gland tumors or about 6 percent of all salivary gland neoplasms .
Clinical Features .

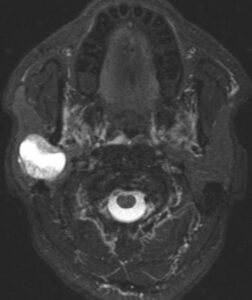
The acinic cell carcinoma closely resembles the pleomorphic adenoma in gross appearance, tending to be encapsulated and lobulated. Although this tumor has been reported occurring chiefly in the parotid, with more than 80 per cent of the cases occurring in the parotid gland, it does occur occasionally in the other major glands and in the accessory intraoral glands. The most common intraoral sites are the lips and buccal mucosa. The acinic cell carcinoma occurs predominantly in persons in middle age or somewhat older, the mean age being 44 years. It has also been encountered in 12 per cent of the patients before the age of 20 years. Women were affected more than men (3: 2). This tumor presents as a slowly growing, mobile or fixed mass of various durations. Usually asymptomatic but pain or tenderness is seen in over a third of the patients. Facial muscle weakness may be seen. Patients with bilateral synchronous tumors have been reported.
Histologic Features.
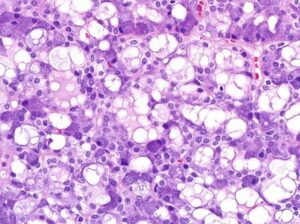
The acinic cell carcinoma, which is frequently surrounded by a thin capsule. may be composed of cells of varying degrees of differentiation. Well-differentiated cells bear remarkable resemblance to normal acinar cells, whereas less differentiated cells resemble embryonic ducts and immature acinar cells. Abrams and his associates have described four growth patterns:
(1) solid,
(2) papillary-cystic,
(3) follicular, and
(4) micro- cystic.
In general, one pattern predominates, although combinations can occur. The most characteristic cell seen has the features of the serous acinar cells, with abundant granular basophilic cytoplasm and a round darkly stained eccentric nucleus. Other cells seen are the intercalated duct like cells, which are smaller and the vacuolated cells which seem to be unique to acinic cell carcinomas among salivary gland neoplasms.
Connective tissue stroma is delicately fibro- vascular collagenous tissue. Lymphoid elements are commonly found in parotid acinic cell carcinomas, a feature which is helpful in the diagnosis. Such features are not found in the intraoral tumors. Apparently the acinic cell carcinoma can arise from embryologically entrapped salivary gland tissue in lymph nodes in or near the parotid compartment. Although ‘clear cells,’ have been described in acinic cell carcinomas, they most likely represent cells altered by fixation or they may actually represent the component cells of a clear cell carcinoma (q.v.), a recently recognized entity .
Treatment and Prognosis.
The treatment of the acinic cell carcinoma in most cases has been surgical. Perzin and LiVolsi recommend total excision of parotid gland tumors with preservation of the facial nerve unless it is involved. Lymph node dissection is indicated only in the presence of clinical involvement and not as a routine procedure. Radiation therapy has not been shown to be of therapeutic value. Intraoral tumors are treated by surgical excision. Poor prognostic features included pain or fixation; gross invasion; and microscopic features of desmoplasia, atypia, or increased mitotic activity. Neither morphologic pattern nor cell composition was a predictive feature.