
Adenoid cystic carcinoma (formerly known as ‘cylindroma’) is a slow-growing but aggressive neoplasm with a remarkable capacity for recurrence, It is characterized by proliferation of ductal (luminal) and myoepithelial cells in cribriform, tubular, solid and cystic patterns. In a review of its case files, the AFIP found adenoid cystic carcinoma to be the fifth most common malignant epithelial tumor of the salivary glands after mucoepidermoid carcinoma; adenocarcinoma, acinic cell carcinoma; and polymorphous low-grade adenocarcinoma (PLGA). However, other series report adenoid cystic carcinoma to be the second most common malignant tumor.
Clinical Features.
The salivary glands most commonly involved by this tumor are the parotid, the submaxillary and the accessory glands in the palate and tongue. The adenoid cystic carcinoma occurs most commonly during the fifth and sixth decades of life, but it is by no means rare even in the third decade. It is seen more commonly in females. Many of the patients exhibit clinical manifestations of a typical malignant salivary gland tumor: early local pain, facial nerve paralysis in the case of parotid tumors, fixation to deeper structures and local invasion. Some of the lesions, particularly the intraoral ones, exhibit surface ulceration. There may be clinical resemblance in some cases to the pleomorphic adenoma. Adenoid cystie carcinoma has a marked tendency to spread through perineural spaces and usually invades well beyond the clinically apparent borders.
Histologic Features.
Adenoid cystic carcinoma is composed of myoepithelial cells and ductal cells which have a varied arrangement.
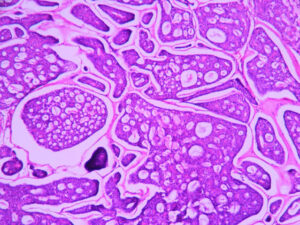
Morphologically, three growth patterns have been described: cribriform (classic), tubular, and solid (basaloid). The tumors are categorized according to the predominant pattern. The cribriform pattern shows basaloid epithelial cell nests that form multiple cylindrical cyst like patterns resembling a swiss cheese or honey comb pattern, which is the most classic and best recognized pattern. The lumina of these spaces contain periodic acid-schiff (PAS) positive mucopolysaccharide secretion. The tubular pattern reveals tubular structures that are lined by stratified cuboidal epithelium. The solid pattern shows solid groups of cuboidal cells with little tendency towards duct or cyst formation. The cribriform pattern is the most common, whereas the solid pattern is the least common. Solid adenoid cystic carcinoma is a high-grade lesion with reported recurrence rates of up to 100 per cent compared with 50-80 per cent for the tubular and cribriform variants.
Variants :
Dedifferentiation of adenoid cystic carcinoma. Dedifferentiated adenoid cystic carcinomas are a recently defined, rare variant of adenoid cystic carcinoma characterized histologically by two components: conventional low-grade adenoid cystic carcinoma and high-grade ‘dedifferentiated’ carcinoma. Because of frequent recurrence and metastasis, the clinical course is short, similar to that of adenoid cystic carcinomas with a predominant solid growth pattern.
Histologically, the low-grade adenoid cystic carcinoma merges gradually into an extensive dedifferentiated component that is composed of solid sheets and cords of anaplastic tumor cells with focal gland formation. Immuno- histochemically, the dedifferentiated component (but not the adenoid cystic carcinoma component) shows strong overexpression of p53 protein and cyclin D1, as well as a higher Ki67 index. Molecular studies confirmed the presence of p53 gene mutation selectively in the dedifferentiated component, suggesting a pivotal role of p53 gene alteration in the dedifferentiation process of adenoid cystic carcinoma.
Treatment and Prognosis.
The treatment of the adenoid cystic carcinoma is chiefly surgical, although in some cases surgery has been successfully coupled with x-ray radiation. Radiation alone is not recommended. In general, this tumor is a slowly growing lesion which tends to metastasize only late in its course. The cure rate for patients with this disease, though varying somewhat from series to series, is discouragingly low. Factors influencing prognosis are the site of occurrence and the histologic pattern of the tumor. Conley and Dingman (1974) found that there is a marked difference in the clinical behavior of major and minor gland adenoid cystic carcinomas. Only 28 per cent of 78 patients with minor gland tumors were alive with no evidence of disease in a four to 14-year follow-up study. Sixty-four per cent of 54 patients with major gland tumors studied over a comparable period were alive and free of disease.