Dens in Dente
It is also called as ‘dens invaginatus’ or ‘dilated composite odontome’ or ‘gestant odontome’. Infolding of the outer surface of the tooth into its interior surface occurs. It is a developmental variation which is thought to arise as a result of an invagination in the surface of crown before calcification.
Etiology
Focal growth retardation there is relative retardation in growth of a portion of the enamel organ, with the result that this part remains stationary and the remainder grows around it.
Active proliferation-another view is that invagination is due to active proliferation of an area of enamel organ which then grows into dental papilla, as a sort of adenoma.
• Increased pressure-study shows that there is presence of extravascular fluid in the soft tissue that fills the potential invagination cavity of the tooth, before it erupts, suggesting that there is increased venous pressure within the invagination. It could be due to pressure on the blood vessels as they pass through the entrance channel of the invagination cavity where enamel is forming concentrically and centripetally, thus tending to progressively narrow the entrance. Expansion of the invagination could then result from the increased venous pressure and transudation.
• Local causes-it can occur due to infection of the deciduous predecessor or trauma. Pressure on the growing teeth can also cause invagination.
Classification
• Coronal dens invaginatus-it is anomalous in folding of enamel organ into dental papilla. It results in folding of hard tissue within the tooth, characterized by enamel lining the fold and covering the dentin peripheral to it.
Radicular dens invaginatus-it is a result of invagination of Hertwig’s epithelial root sheath resulting in accentuation of normal longitudinal root grooves. It is lined by cementum. Root sheath may bud off sac like invagination, that results in a circumscribed cementum defect in root.
Clinical features
Coronal dens invaginators
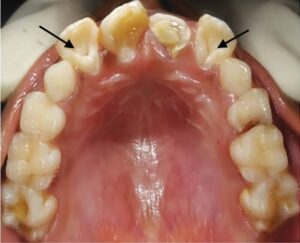
Site-commonly affected tooth is permanent maxillary lateral incisor and maxillary central incisor. The lower incisor or cuspid is the next common site. No sexual predilection.
Age and sex-it is diagnosed in children or in adolescents. It is more common in females.
Occurrence-this condition is frequently bilateral.
Mild form–there is a deep pit in cingulum.
Moderate
Pocket of enamel is formed within tooth, with – dentin at periphery.
Opening to the surface is constricted or remains open.
• Food debris may become packed in this area with resultant caries and infection of pulp.
Severe form-it may exhibit an invagination extending nearly to the apex of the root.
Crown features
The crown may or may not be enlarged.
The shape of crown may be conical or it may be of irregular shape.
Appearance
In some cases there appears to be a grossly magnified cingulum rising to the level of the incisive edge of the tooth, but lacking the normal contour of a cingulum.
The labial face of the tooth is often bulbous. Some teeth with these abnormalities are son misshapen as to defy verbal description.
Radicular dens invaginatus
Site-it is more common in 1st mandibular premolar, upper lateral incisor and second molar. Abnormality is usually unilateral. It occurs most frequently at the site of anatomical defect.
Crown features-crown is small, short and conicala with small orifice at the extreme summit of the convexity. Lingual marginal ridge is prominent.
Cavity is separated from the pulp chamber by a thin wall and opens in oral environment through very narrow constriction
Radiographic features

Coronal dens invaginators
Radiodensity-infoldings is recognized by its greater radiodensity.
Size-it may vary in size from very small and superficial, to large and deep.
Apical area-it is common for the apical portion of the canal to diverge.
Pulp chamber-in addition to small but otherwise normal pulp chamber there is sometimes an additional cavity of variable shape and size which may be separated from real pulp chamber or may unite with it.
Radicular dens invaginators
Radiodensity-radicular invagination will appear as a poorly defined, slightly radiolucent structure running longitudinally within the root.
Appearance-the root is composed of a saucer shaped expansion, the concavity of which represents the dilated feature of the tooth.
Inverted open umbrella-the tooth resembles ‘inverted open umbrella’, the handle of which is short, being represented by the conical, nipple shaped crown.
Size-the diameter of expanded portion of the root. at the extreme apex is as much as 2 cm.
Apical foramina-apical foramina of the root is wide.
There is always area of radiolucency present in the bone at the end of the radicular portion as a result of rarefying osteitis, which has followed the passage of organism from the mouth upto the canal in the tooth.
Histopathological features
The lining consist of enamel and at the opening of the cavity this is continuous with the enamel that covers the exterior of the tooth.
In invagination of severe type, pulp cavity is grosslys encroached upon and may be represented by a mere slit in the dentine on each side of the invagination cavity
Enamel lining is defective owing to poor mineralization and may be totally absent in the area.
Management
Tooth should be restored prophylactically