Apollo Hospital Senior Associate Dental Surgeon
Ex ITBP Hospital Senior Dental Surgeon
Senior Dental Surgeon at Parthsarathy Painless Dental Clinic Shivpuri
Ex Dental Surgeon & Lecturer at Mansarovar Hospital & Research Center Bhopal
Senior Dental Surgeon & Healthcare Consultant at Practo
Diastema Closure

A maxillary midline diastema is often complicated by the insertion of the labial frenum into a notch in the alveolar bone, so that a band of heavy fibrous tissue lies between the central incisors. When this is the case, a stable correction of the diastema almost always requires surgery to remove the interdental fibrous tissue and reposition the frenum. The frenectomy must be carried out in a way that will produce a good esthetic result and must be properly coordinated with orthodontic treatment.
It is an error to surgically remove the frenum at an early age and then delay orthodontic treatment in the hope that the diastema will close spontaneously. If the frenum is removed while there is still a space between the central incisors, scar tissue forms between the teeth as healing progresses, and a long delay may result in a space that is more difficult to close than it was previously.
It is better to align the teeth before frenectomy. Sliding them together along an arch wire is usually better than using a closing loop because a loop with any vertical height will touch and irritate the frenum. If the diastema is relatively small, it is usually possible to bring the central incisors completely together before surgery. If the space is large and the frenal attachment is thick, it may not be possible to completely close the space before surgical intervention. The space should be closed at least partially, and the orthodontic movement to bring the teeth together should be resumed immediately after the frenectomy, so that the teeth are brought together quickly after the procedure. When this is done, healing occurs with the teeth together, and the inevitable postsurgical scar tissue stabilizes the teeth instead of creating obstacles to final closure of the space.”
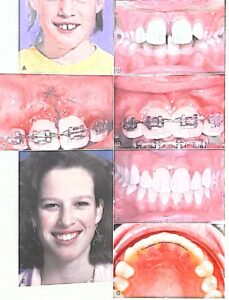
Management of a maxillary midline diastema.
A, Facial appearance, showing the protruding maxillary incisors caught on the lower lip.
B, Intraoral view before treatment.
C, Teeth aligned and held tightly together with a figure-8 wire ligature, before frenectomy.
D, Appearance immediately after frenectomy, using the conservative technique advocated by Edwards in which a simple incision is used to allow access to the interdental area, the fibrous connection to the bone is removed, and the frenal attachment is sutured at a higher level.
E, Facial appearance 2 years after completion of treatment.
F, Intraoral view 2 years after treatment.
G, Bonded retainer, made with .0175 steel twist wire. It is important for the wire to be flexible enough to allow some displacement of the incisors in function-a rigid wire is much more likely to break loose.
The key to successful surgery is removal of the interdental fibrous tissue. It is unnecessary and, in fact, undesirable to excise a large portion of the frenum itself. Instead, a simple incision is used to allow access to the interdental area, the fibrous connection to the bone is removed, and the frenum is then sutured at a higher level.”
A maxillary midline diastema tends to recur, no matter how carefully the space was managed initially. The elastic gingival fiber network typically did not cross the midline in these patients, and the surgery interrupted any fibers that did cross. As a result, in this critical area the normal mechanism to keep teeth in contact is missing. A bonded fixed retainer is recommended.
Causes Of Diastema
The size of the teeth in relation to the jawbone
If a person’s teeth are too small, relative to the size of their jawbone, gaps may develop between the teeth.
Jawbone and tooth sizes can be genetic, which is one reason that diastemas can run in families.
Missing or undersized teeth
If some teeth are missing or smaller than others, a diastema can develop.
This often involves the upper lateral incisors — the teeth to either side of the two upper front teeth. If the upper lateral incisors are missing or relatively small, a gap can develop between the two front teeth.
Oversized labial frenum
The labial frenum is the tissue that extends from the inside of the upper lip to the gum above the upper front teeth.
If this tissue is especially large, it can cause a gap to form between these teeth.
Gum disease
Tooth migration is a typical sign of advanced gum disease.
In people with gum disease, inflammation results in damage to the bone that supports the teeth.
Eventually, the teeth may become loose, and gaps can appear.
Incorrect swallowing reflex
When the swallowing reflex happens correctly, the tongue presses against the roof of the mouth.
A person may instead push their tongue against their front teeth when they swallow. Over time, this repetitive pressure against the front teeth pushes them forward, causing a gap to form.
Habits
Thumb sucking, lip sucking, tongue thrusting, and similar habits can put pressure on the front teeth, pushing them forward.
This can lead to diastemas.
Loss of primary teeth
Children can develop temporary diastemas when their primary teeth, or baby teeth, fall out. When their permanent, or adult, teeth come in, these gaps typically close.
This type of gap is common Trusted Source enough that dentists consider it to be a normal developmental phenomenon in children. No treatment is usually necessary.