
As per the WHO, diabetes mellitus (DM) is a hetro- geneous metabolic disorder characterised by common feature of chronic hyperglycaemia with disturbance of carbohydrate, fat and protein metabolism.
DM is a leading cause of morbidity and mortality the world over. It is estimated that approximately 1% of population offers from DM. The incidence is rising in the developed countries of the world, especially of type 2 DM, due to rising incidence of obesity and reduced activit levels. DM is expected to continue as a major health problem owing to its serious complications, especially end-stage renal disease, IHD, gang- rene of the lower extremities and blindness in the adults.
CLASSIFICATION AND ETIOLOGY :
The older classification systems dividing DM into primary (idiopathic) and secondary types, juvenile-onset and maturity onset types, and insulin-dependent (IDDM) and non-insulin dependent (NIDDM) types, have become obsolete and undergone major revision due to extensive understanding of etiology and patho- genesis of DM in recent times.
Based on etiology, currently DM is classified into two broad categories (type 1 and type 2),
Etiological Classification of Diabetes Mellitus
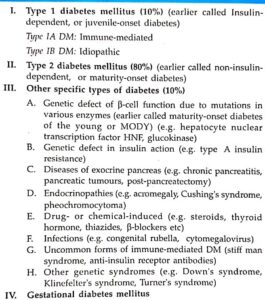
a few uncommon specific etiologic types, and gestational DM. Brief comments on these etiologic terminologies as contrasted with former nomenclatures of DM are given below:
TYPE 1 DM. It constitutes about 10% cases of DM. It was previously termed as juvenile-onset diabetes (JOD) due to its occurrence in younger age, and was called insulin-dependent DM (IDDM) because these patients had absolute requirement for insulin replacement as treatment. However, in the new classification, neither age nor insulin-dependence are considered as absolute criteria. Instead, based on underlying etiology, type 1 DM is further divided into 2 subtypes:
Subtype 1A (immune-mediated) DM characterised by autoimmune destruction of B-cells which usually leads to insulin deficiency.
Subtype 1B (idiopathic) DM is characterised by insulin deficiency with tendency to develop ketosis but these patients are negative for autoimmune markers.
Though type 1 DM occurs commonly in patients under 30 years of age, autoimmune destruction of B- cells can occur at any age. In fact, 5-10% patients who develop DM above 30 years of age are of type 1A DM and hence the term JOD has become obsolete.
TYPE 2 DM. This type comprises about 80% cases of DM. It was previously called maturity-onset diabetes, or non-insulin dependent diabetes mellitus (NIDDM) of obese and non-obese type.
Although type 2 DM predominantly affects older individuals, it is now known that it also occurs in obese adolescent children; hence the term MOD for it is inappropriate. Moreover, many type 2 DM patients also require insulin therapy to control hyperglycaemia or to prevent ketosis and thus are not truly non-insulin dependent contrary to its former nomenclature.
The contrasting features of Type 1 & Type 2 Diabetes Mellitus
OTHER SPECIFIC ETIOLOGIC TYPES OF DM :
Besides the two main types, about 10% cases of DM have a known specific etiologic defect. One important subtype in this group is maturity-onset diabetes of the young (MODY) which has autosomal dominant inheritance, early onset of hyperglycaemia and impaired insulin secretion.
GESTATIONAL DM :
About 4% pregnant women develop DM due to metabolic changes during preg- nancy. Although they revert back to normal glycaemia after delivery, these women are prone to develop DM later in their life.
Contrasting Features of Type 1 & Type 2 Diabetes Mellitus

CLINICAL FEATURES :
It can be appreciated that hyperglycaemia in DM does not cause a single disease of is associated with numerous diseases and symptons, especially due to complications. Two main types of DM can be distinguished clinically. However, overlapping of clinical features occurs as regards the age of onset, cution of symptoms and family history.
Pathophysiological basis of common signs and symptoms due to uncontrolled hyperglycaemia in diabetes mellitus

Type 1 DM:
i) Patients of type 1 DM usually manifest at early age, generally below the age of 35.
ii) The onset of symptoms is often abrupt.
iii) At presentation, these patients have polyuria,
polydipsia and polyphagia.
iv) The patients are not obese but have generally progressive loss of weight.
v) These patients are prone to develop metabolic complications such as ketoacidosis and hypoglycaemic episodes.
Type 2 DM:
i) This form of diabetes generally manifests in middle life or beyond, usually above the age of 40.
ii) The onset of symptoms in type 2 DM is slow and insidious.
iii) Generally, the patient is asymptomatic when the diagnosis is made on the basis of glucosuria or hyper- glycaemia during physical examination, or may present with polyuria and polydipsia.
iv) The patients are frequently obese and have unexplained weakness and loss of weight.
v) Metabolic complications such as ketoacidosis are infrequent.