
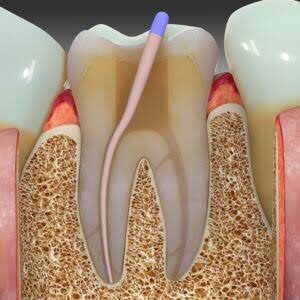
Root canal therapy may be defined as the complete removal of the irreversibly damaged dental pulp followed by thorough cleaning, shaping and filling of the root canal system that the tooth may remain as a functional unit with in the dental arch . The rationale of root canal treatment relies on the fact that the nonvital pulp, being avascular, it has no defense mechanisms. The damaged tissue within the root canal undergoes autolysis and the resulting break down products will diffuse into the surrounding tissues and cause periapical irritation associated with the portals of exit even in the absence of bacterial contamination. The complex anatomy of the apical delta of many root canals makes complete debridement virtually impossible. It is essential therefore, that endodontic therapy must include sealing of the root canal system to prevent tissue fluids from percolating in the root canal and prevent toxic by-products from both necrotic tissue and microorganisms regressing into the periradicular tissues.
The current accepted method of obturation of prepared canals employs a solid or a semisolid core such as gutta- percha and a root canal sealer. Gutta-percha has no adhesive qualities to dentin regardless of the obturation technique used. Therefore root canal sealers along with solid core play a major role in achieving the hermetic seal by filling the accessory root canals, voids, spaces and irregularities and hence reducing the chances of failure of root canal treatment.
Not all teeth with positive bacterial cultures fail, nor do all teeth with negative cultures succeed. Thus entombing residual microorganisms and irritants by sealing them within the root canal system may have a major influence on clinical outcome. Leakage of fluids through an obturated root canal can occur between the sealer and dentin, the sealer and gutta-percha, or through the voids with in the sealer . Although sealers enhance sealing ability by filling in any residual spaces and bonding to dentin, the optimal outcome of obturation is to maximize the volume of the core material and minimize the amount of sealer between the inert core and the canal wall.
Thus we can say that a three dimensional well fitted root canal with fluid tight seal is the main objective of the root canal obturation. It serves the following:
a) Prevents percolation and microleakage of periapical exudate into the root canal space.
b) Prevents infection by completely obliterating the apical foramen and other portals of communication.
c) Creates a favorable environment for process of healing to take place.
LATERAL COMPACTION TECHNIQUE :
It is one of the most common methods used for root canal obturation. It involves placing tapered gutta-percha cones in the canal and then compacting them under pressure against the canal walls using a spreader. A canal should have continuous tapered shape with a definite apical stop. before it is ready to be filled by this method .
Technique :
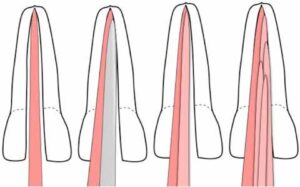
1. Following the canal preparation, select the master gutta- percha cone whose diameter is consistent with largest file used in the canal up to the working length. One should feel the tugback with master gutta-percha point . master gutta-percha point is notched at the working distance analogous to the level of incisal or occlusal edge reference point .

2. Check the fit of cone radiographically. If found satisfactory, remove the cone from the canal and place it in sodium hypochlorite. If cone fits short of the working length, check for dentin chip debris, any ledge or curve in the canal and treat them accordingly and
If cone selected is going beyond the foramen, either select the larger number cone or cut that cone to the working length .
If cone shows “s” shaped appearance in the radiograph that means cone is too small for the canal. Here a larger cone must be selected to fit in the canal.
3. Select the size of spreader to be used for lateral compaction of that tooth. It should reach 1-2 mm of true working length .
4. Dry the canal with paper points and apply sealer in the prepared root canal .
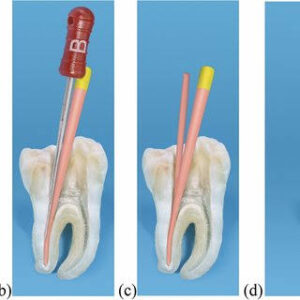
5. Now premeasured cone is coated with sealer and placed into the canal. After master cone placement, spreader is placed into the canal alongside the cone. Spreader helps in compaction of gutta-percha. It act as a wedge to squeeze the gutta-percha laterally under vertical pressure not by pushing it sideways . It should reach 1-2 mm of the prepared root length.
6. After placement, spreader is removed from the canal by rotating it back and forth. This compacts the gutta- percha and a space gets created lateral to the master cone .
7. An accessory cone is placed in this space and the above procedure is repeated until the spreader can no longer penetrate beyond the cervical line.
8. Now sever the protruding gutta-percha points at canal orifice with hot instrument .
Advantages of Lateral Compaction Technique :
1. Can be used in most clinical situations.
2. During compaction of gutta-percha, it provides length control, thereby prevent overfilling.
Disadvantages :
1. May not fill the canal irregularities efficiently.
2. Does not produce homogenous mass.
3. Space may exist between accessory and master cones .