CLASSIFICATION OF OROFACIAL PAIN
Pain may be classified by various criteria such as

Anatomical location
Etiology
Neurophysiological mechanism
Neural pathway that mediates the sensation
Temporal behavior
Clinical characteristics
FIRST CLASSIFICATION
Neuropathic Pain
Orofacial pain associated with clinically demonstrated nerve dysfunction or observed abnormalities of the peripheral nerve.
Paroxysmal pain of neuropathic origin
Trigeminal neuralgia
Geniculate neuralgia
Glossopharyngeal neuralgia
Nonparoxysmal pain of neuropathic origin
Post-traumatic pain
Post-viral orofacial pain
Neoplasm of the parotid gland, nasopharynx and acoustic neuroma
Non-neuropathic Pain
It is the orofacial pain in absence of disease primarily involving those nerves likely to be associated with the pain. It is subdivided into:
Non-neuropathic pain of central origin
In separating pain into neuropathic and non- neuropathic categories the entrance point of the dorsal root of the cranial nerve into the brain is chosen as the dividing line between peripheral and central nervous systems. Pain caused by the lesions affecting the intracranial but extra-pontine or extramedullary portion of cranial nerves V, VII, IX, and X is classified as neuropathic and that caused by the lesions affecting the cord (central nervous system) is referred to as non- neuropathic pains of central origin.
Neuronal damage-orofacial pain of central origin is thought to result from neuronal damage in CNS secondary to traumatic injury to peripheral nerves.
• Phantom limb pain-phantom limb pain and causalgia (a persistence burning sensation resulting from peripheral nerve trauma associated with various other phenomenon )
Brain tumor and central lesion-tumor, vascular lesion and other destructive lesions of the brain- stem, pons, thalamus and cerebrum should be considered in the diagnosis of chronic orofacial pain.
Other causes like thalamic syndrome of Dejerine and Roussy, tertiary neurosyphilis and multiple sclerosis.
Non-neuropathic pain of extraneural origin
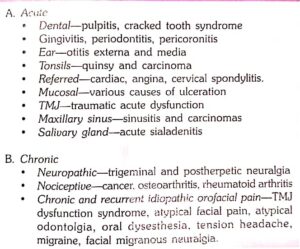
Dental-this includes dental caries, exposed dentin and cementum, pulpal and periapical disease, periodontal disease, pericoronitis, impacted food, ANUG, faulty restorations, fractured teeth, traumatic occlusion, tooth eruption and exfoliation, unerupted and impacted teeth, retained root, dental cyst, postsurgical pain, post-injection pain and other direct trauma to the teeth and aerodontalgia.
Alveolar and adjacent tissue origin-dry socket, sinusitis, various neoplastic and non-neoplastic osteolytic lesions, Paget’s disease, multiple myeloma etc.
Musculoskeletal TMJ arthritis, TMJ myofacial dysfunction, myositis, muscle spasm and trismus, cervical muscle spasm, osteoarthritis, arthralg0aia of the cervical spine and tension headache.
Vascular-vascular headaches including migraine and cluster headache, toxic and metabolic vascular headache, hypertensive vascular changes, arterial diseases such as aneurysms, emboli, cranial arteritis (including giant cell arteritis, polymyalgia and immune arteritis). thrombophlebitis and carotidynia.

Pain referred from outside the orofacial area- otitis media, inflammatory or neoplastic diseases of the ear, diseases of major salivary glands (calculus, cyst and tumor), lesions of nasal and sinus mucosa, myocardial ischemia which may cause pain in the orofacial area, often at some distance from the focus of disease.
Pain of Unknown Nature

Pain that arises outside the peripheral nerve and only affects the nerves and their receptors secondarily (e.g. pain of dental caries, periodontal disease and mouth ulcers).