
Cystadenocarcinoma is the malignant counterpart of cystadenoma. It is a rare malignant epithelial tumor characterized histologically by prominent cystic and, frequently, papillary growth but lacking features that characterize cystic variants of several more common salivary gland neoplasms.
Clinical Features.
Cystadenocarcinoma is considered to be a low-grade neoplasm. Most of the cases, about 65 per cent, occurred in the major salivary glands (primarily in the parotid). Among the reported cases men and women are found to be affected equally and the average age at presentation is about 59 years. Patients present with a slowly growing asymptomatic mass. Clinically, this neoplasm is rarely associated with pain or facial paralysis.
Histologic Features.
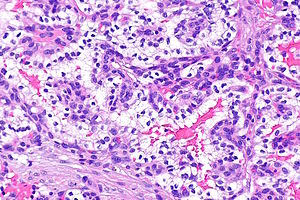
A cystic growth pattern must dominate the histologic appearance for the diagnosis to be considered. These cystic spaces vary in size between tumors as well as within the same tumor. These neoplasms may appear circumscribed or reveal haphazard growth throughout the gland. The lumina often are filled with mucus and hemorrhage and dystrophic calci- fications are sometimes evident focally. The lining cells vary from cuboidal to tall columnar, and often a single tumor contains basaloid, oncocytic, clear, and occasionally, mucus cells that form adenomatous or nodular, solid epithelial areas. These solid areas usually occupy the space between the cystic structures.
Nuclear hyperchromatism and nuclear variability are subtle, and only rare mitotic figures are present. Nucleoli may be obvious. Encapsulation is incomplete, and infiltration into either salivary gland parenchyma or fibrous or adipose tissue is seen. The tumor may infiltrate either as cyst like structures or as solid islands. Although the vast majority of cystadenocarcinomas are low- grade lesions, moderate/intermediate grade tumors do exist.
Treatment and Prognosis.
No information is currently available that pertains specifically to the prognosis of the salivary gland cystadenocarcinomas. Currently the treatment principles for low- grade cystadenocarcinomas are similar to the principles applied for other low-grade salivary gland adenocarcinomas. These include consideration of the site, the clinical extent of the disease and the histologic grade prior to institution of therapy. Radical neck dissection should be preserved only to deal with obvious metastases.