 Polymorphous low-grade adenocarcinoma (PLGA) is a malignant epithelial tumor that is essentially limited in occurrence to minor salivary gland sites and is characterized by bland, uniform nuclear features; diverse but characteristic architecture; infiltrative growth; and perineural infiltration. This is a recently recognized type of salivary gland tumor first described in 1983. Evans and Batsakis first used the term polymorphous low-grade adenocarcinoma in 1984 to describe this tumor. This tumor includes those entities, which were previously termed as terminal duct carcinoma, lobular carcinoma, papillary carcinoma and trabecular carcinoma.
Polymorphous low-grade adenocarcinoma (PLGA) is a malignant epithelial tumor that is essentially limited in occurrence to minor salivary gland sites and is characterized by bland, uniform nuclear features; diverse but characteristic architecture; infiltrative growth; and perineural infiltration. This is a recently recognized type of salivary gland tumor first described in 1983. Evans and Batsakis first used the term polymorphous low-grade adenocarcinoma in 1984 to describe this tumor. This tumor includes those entities, which were previously termed as terminal duct carcinoma, lobular carcinoma, papillary carcinoma and trabecular carcinoma.
Clinical Features.
In minor gland sites polymorphous low-grade adenocarcinoma is twice as frequent as adenoid cystic carcinoma, and, among all benign and malignant salivary gland neoplasms, only pleomorphic adenoma and mucoepidermoid carcinoma are more common. The average age of patients is reported to be 59 years, with 70 per cent of patients between the ages of 50 and 79 years. The female to male ratio is about 2: 1. In the AFIP case files, over 60 percent of tumors occurred in the mucosa of either the soft or hard palates, approximately 16 per cent occurred in the buccal mucosa, and 12 percent in the upper lip. Polymorphous low-grade adenocarcinoma typically presents as a firm, nontender swelling involving the mucosa of the hard and soft palates (often at their junction), the check, or the upper lip. Discomfort, bleeding, telangiectasia, or ulceration of the overlying mucosa may occasionally occur.
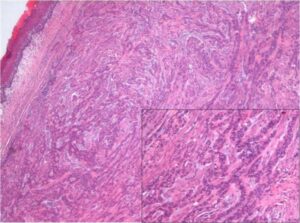
Histologic Features.
Microscopically polymorphous low-grade adenocarcinoma is characterized by infiltrative growth with diverse morphology and uniform cytologic features. The tumors are well circumscribed but unencapsulated and infiltrate into adjacent structures. The polymorphic nature of the lesion refers to the variety of growth patterns it assumed which includes solid, ductal, cystic and tubular. In some tumors, a cribriform pattern can be produced, which resembles adenoid cystic carcinoma. The tumor is composed of cuboidal to columnar isomorphic cells that have uniform ovoid to spindle shaped nuclei. Scant to moderate amounts of eosinophilic cytoplasm can be seen. The tumor stroma varies from mucoid to hyaline and in some cases, tumor nests are separated by fibrovascular stroma. Perineural invasion is common that makes this tumor mistaken as adenoid cystic carcinoma.
Treatment.
Polymorphous low-grade adenocarcinoma is best treated by conservative wide surgical excision. This neoplasm typically runs a moderately indolent course. Although the tumor can recur, sometimes multiple times over many years, distant metastases have not been reported. The overall prognosis is good. Perineural invasion does not appear to affect the prognosis.