It is chronic progressive damage or loss of tooth structure due to the action of cells called odontoclasts. It can be physiological as in case of root resorption of deciduous teeth or pathological, which occurs in permanent teeth. Pathological resorption may be external or internal.
EXTERNAL RESORPTION :-
It is lytic process occurring in the cementum or cementum and dentin of the roots of teeth.
Types :-
•Resorption occurring at the apex or along the lateral surface of the root.
• External internal resorption.
Etiology :-
Resorption associated with periapical infection- periapical granuloma (arising due to pulpal infection or trauma), causes subsequent resorption of root apex. On the radiograph, it appears as slight raggedness or blunting of the root apex in the early stages.
Reimplanted teeth-It may result in severe resorp- tion of root. Tooth root is resorbed and replaced by bone which produces ankylosis. Many implanted teeth exhibit complex resorption of root and are gradually exfoliated.
Tumors and cysts-resorption due to tumors and cysts appears to be essentially by pressure phenomenon. In most cases, tissue is present between the tumor and the tooth and it is from this tissue that cells, chiefly osteoclasts arise and initiated root resorption. Cysts like apical periodontal cyst may exert such pressure on the apex of tooth that the intervening connective tissue may in turn get stimulated for osteoclasts formation and thus. resorption begins. The apex may be lost leaving a flat or scalloped surface at the distal end of the root.
Excessive mechanical and occlusal forces-usually, due to the force that is applied during orthodontic treatment, the patient exhibits multiple areas of root resorption, irrespective of the manner of treatment. Pressure from occlusal forces results in destruction, primarily of bone, then small lacunae often appear on the surface of cementum and ultimately, it extends into the dentin.
Impacted teeth-teeth which are completely impacted or embedded in the bone, occasionally, will undergo resorption of the crown and root. Impacted tooth also may cause resorption of roots of adjacent teeth without itself getting resorbed. This is commonly seen in case of horizontally or mesioangularly impacted mandibular 3rd molars impinging on roots of 2nd molar.
Overhanged root canal filling material-in such cases not only the apex get resorbed but more or less, sides of the root are affected. In some cases, all or most of the root disappears and the regenerating bone eventually embraces the root canal filling intimately, so that it appears as if the crown of the tooth is held in position by the root filling.
Idiopathic-in this case, burrowing type of external resorption can occur which is usually seen in relation with single or multiple erupted teeth.
CLINICAL FEATURES
Symptoms the affected tooth is usually asympto- matic.
• Sites the most frequent site for external resorption is upper incisors, upper and lower bicuspids. .
Signs :-
• When the root is completely resorbed, the tooth may become mobile.
• If root resorption is followed by ankylosis then the tooth is immobile, in infraocclusion and with high percussion sound.
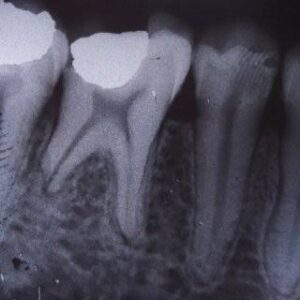
Radiographic Features :-
External resorption
• When the lesion begins at the apex, it causes smooth resorption of the root surface. The conical end is removed and replaced by more or less blunt or usually square apex.
•Bone and lamina dura show normal appearance. It appears as concave and ragged area on the root surface.
• If it involves lateral aspect of the tooth, the lesion will be irregular.
External-internal resorption :-
• It appears as eccentrically shaped notch with areas of resorption which are uneven and appears like trabeculae.
Histopathological Features :-
• It is the result of osteoclastic activity on the root surface of the involved tooth.
•Microscopically it varies from small area of cementum resorption replaced by connective tissue or repaired by new cementum; too large areas of resorption are replaced by osseous tissues and ‘scooped out’ areas of resorption are replaced by inflammatory or neoplastic tissue.
Differential Diagnosis :-
Internal resorption-in external resorption, the radiograph shows blunting of the apex, a ragged area, a scooped out area on the side of the root. In internal resorption, one can see root canal with well demarcated enlarged ballooning area of resorption. It appears as expansion of pulp chamber and canals.
•Incomplete root formation-in it, incomplete canal diverges, whereas in external resorption, they usually converges
•Short root-it has conical apex and the root canal is usually not visible at the extreme apex nor is the foramen.
•Apicectomy-it revels evidence of root filling and the history is available.
•Foreshortening of root-despite the short root, the canal at the apical end cannot be seen and neither can be the foramen.
Management :-
•Apicoectomy
•If the area is broad and on lateral surface, curettage and filling of resorbed area should be carried out.
INTERNAL RESORPTION :-
It begins certainly in the tooth. It is a condition starting in the pulp, in which the pulp chamber or the root canals or both, of the tooth expand by resorption of the surrounding dentin.
*It is an idiopathic, slow or fast progressive resorptive process occurring in the dentin or pulp chamber or root canals.
Etiology :-
•Idiopathic
•Inflammatory hyperplasia of the pulp
•Direct and indirect pulp capping
•Pulpotomy
•Enamel invagination
•Acute trauma to teeth
•Pulp polyp
Mechanism :-
Precipitating factor→ vascular changes in pulp → inflammation and production of granulation tissue →→ metaplasia of embryonic connective tissue and macrophages → odontoclast like giant multinuc- leated cells resorption of internal wall of pulp.
Types :-
• Internal inflammatory resorption-it occurs due to intense inflammatory reaction within the pulp tissue.
•Internal replacement resorption-it occurs in absence of any inflammatory reaction within the pulp.
Clinical Features :-
Appearance-appearance of pink hued area on the crown of tooth, which represents hyperplastic pulp tissue fitting the resorbed area and showing through the remaining overlying tooth substance.
• Teeth involved :
•It may affect any tooth in primary and secondary dentitions, with prevalence in permanent dentition.
• It is more common in central incisor, lateral incisors, premolar and canine and 3rd molar according decreasing frequency.
• Multiple tooth involvement may be there.
•Age and sex-it occurs during 4th and 5th decades of life and is more common in males.
Symptoms-it is asymptomatic.
•Pink spot-the roots of teeth with internal resorption may manifest a reddish area, called the ‘pink spot”. This reddish area represents granulation tissue showing through the resorbed area of crown.
Signs :-
•When the lesion is located in the crown of teeth, it may expand to such an extent that the crown shows dark shadow due to necrosis of the pulp tissue.
• If the resorption is in the root, it may weaken the tooth and result in fracture of the tooth.
•Infectious pulpitis-it may perforate the crown with hemorrhagic tissue projecting from the perforation and result in infectious pulpitis.
Radiographic Features :-
•Appearance lesion is radiolucent, round, oval or elongated within the root with widening of pulp chamber or canals.
•Location-the destruction may be symmetrically situated around the original canal or it may be eccentric, so that it is situated entirely on one side of the root.
•Shape the tooth substance which is destroyed in the root may assume any shape; rounded, oval, inverted, pear or irregular.
•Margins-the margins of enlarged chamber are sharp and clearly defined.
•Internal structure-radiolucency is homogenous without bony trabaculation or radiopaque foci. Outline of the lesion is sharply defined and smooth or slightly scalloped.
Histopathological Features :-
•Resorption of the inner or pulpal surface of dentin and proliferation of the pulp tissue, filling the defect.
•It may show occasional osteoclasts or odontoclasts hence it is called as odontoclastoma.
•Pulp tissue usually exhibits chronic inflammatory reaction.
•Alternating periods of resorption and repair are manifested as irregular lacunae like areas in dentin that are partially or completely filled with irregular dentin or osteodentin.
•When the root surface is perforated, it is very difficult to determine whether the lesion began externally on internally.
•Multinucleated giant cells and odontoclast are also present.
Differential Diagnosis :-
•Dental caries-carious lesion show more diffused margins than internal root resorption. In most cases of internal resorption, enamel is not involved so. there is no evidence of external orifice.
•External resorption-in internal resorption, defect is more extensive in the pulpal wall than on the root surface.
Management :-
•Extirpation of pulp with routine endodontic treatment or retrograde filling stops the internal resorption process.
•Extraction of the tooth, if perforation occurs.