Tooth Structure and Toothache
The basic structure of tooth is made up of :-
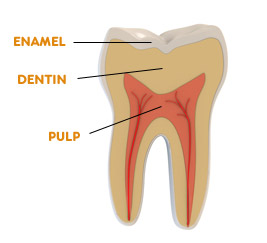
Enamel
Enamel forms a protective covering of variable thickness over the entire surface of the tooth crown. On the cusps of human molars and premolars the enamel attains a maximum thickness of about 2 to 2.5 mm, thinning down to almost a knife edge at the neck of the tooth.
The tooth structure and contour of the cusps receive their final modeling in the tooth enamel. Because of its high content of mineral salts and their crystalline arrangement, enamel is the hardest calcified tissue in the human body. The function of the enamel is to form a resistant covering of the tooth structure from bacterial attack protecting from toothache, rendering them suitable for mastication.
Tooth Structure and Toothache
white, It has been suggested that the tooth color is determined by differences in the translucency of enamel, yellowish teeth having a thin, translucent enamel through which the yellow color of the dentin is visible and grayish teeth having a enamel. The translucency may be attribute- able to variations in the degree of calcification and homogeneity of the enamel. If decay starts in enamel some patients complaints toothache in the form of sensitivity.
Grayish tooth structure frequently show a slightly yellowish color at the cervical areas, presumably because the thinness of the enamel permits the light to strike the underlying yellow dentin and be reflected. Incisal areas may have a bluish tinge where the thin edge consists only of a double layer of enamel.
Dentine
The dentin provides the bulk and general form of the tooth structure and is characterized as a hard tissue with tubules throughout its thickness. Since it begins to form slightly before the enamel, it determines the tooth structure shape of the crown, including the cusps and ridges, and the number and size of the roots.
Tooth Structure and Toothache
In the teeth of young individuals the dentin usually is light yellowish in color, becoming darker with age. Unlike enamel, which is very hard and brittle, dentin is viscoelastic and subject to slight deformation. It is somewhat harder than bone but considerably softer than enamel. Dentin hardness varies slightly between tooth types and between crown and root dentin.
Dentin is somewhat harder in its central part than near the pulp or on its periphery. If bacteria crosses dentine of tooth structure and reach in pulp toothache can starts. The dentin of primary teeth is slightly less hard than that of permanent teeth. The lower content of mineral salts in dentin renders it more radiolucent than enamel. Dentin consists of 35% organic matter and water and 65% inorganic material.
Pulp
The dental pulp occupies the center of each tooth structure and consists of soft connective tissue.
The central region of both the coronal and the radicular pulp contains large nerve trunks and blood vessels in which bacteria develop faster leads to toothache.
The primary role of the pulp anlage is to interact with the oral epithelial , cells, which leads to differentiation of the dental lamina and enamel organ formation.
Tooth Structure and Toothache
The pulp anlage also interacts with the developing enamel organ as it determines a particular type of tooth structure.
The pulp organ cells produce the dentin that surrounds and protects the pulp from inflammation and toothache. The pulpal odontoblasts develop the organic matrix and function in its calcification.
The pulp nourishes the dentin through the odontoblasts and their pro- cesses and by means of the blood vascular system of the pulp.
The sensory nerves in the tooth structure respond with pain to all stimuli such as toothache, heat, cold, pressure, operative cutting procedures, and chemical agents.
The pulp is an organ with remarkable reparative abilities. The pulp has macro- phages, lymphocytes, neutrophils, mono- cysts, and plasma and mast cells, all of which aid in the process of repair of the pulp of tooth structure, protect from bacterial attacks and prevents toothache.
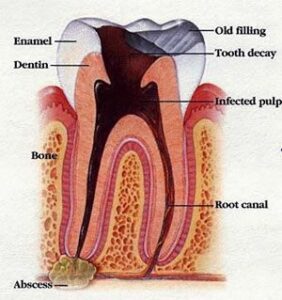
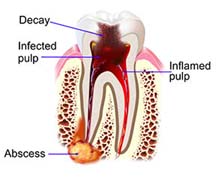
DISEASES OF DENTAL PULP OF TOOTH STRUCTURE AND TOOTHACHE
The dental pulp of tooth structure is a delicate connective tissue liberally interspersed with tiny blood vessels, lymphatics, myelinated and unmyelinated nerves, and undifferentiated connective tissue cells, it reacts to bacterial infection or to other stimuli by an inflammatory response known as pulpitis, which is the most common cause of odontalgia or toothache.
ETIOLOGIC FACTORS IN PULP DISEASE
Most cases of pulpitis are primarily a result of dental caries in which bacteria or their products invade the dentin and pulp tissue of tooth structure.
Occasionally, there is bacterial invasion in the absence of caries, as in cases of tooth fracture due to trauma or cracked tooth syndrome in tooth structure that expose the dental pulp to the oral fluids and microorganism leads to toothache. In cracked tooth syndrome, a tooth, particularly a restored premolar may split, usually under masticatory stress. These cracks are often minute and invisible clinically, and they allow the bacteria into the pulp of tooth structure causing toothache. Bacterial invasion may also occur as a result of a bacteremia and septicemia.
Bacteria circulating in the blood stream tend to settle out or accumulate at sites of pulpal inflammation, such as that which might follow some chemical or mechanical injury to the pulp tooth structure. They termed this particular phenomenon as ‘anachoretic pulpitis’ leads to toothache. Anachoresis is a phenomenon by which blood borne bacteria, dyes, pigments, metallic sub- stances, foreign proteins, and other materials are attracted to the site of inflammation.
Focal Reversible Pulpits
A tooth structure with focal pulpitis is sensitive to thermal changes, particularly to cold. The application of ice or cold fluids to the tooth results in toothache, but this disappears upon removal of the thermal irritant or restoration of the normal temperature. It will be found also that such a tooth responds to stimulation by the electric pulp tester at a lower level of current, indicating a lower toothache threshold (or a greater sensitivity) than that of adjacent normal tooth structure.
Tooth structure in which this condition exists usually show deep carious lesions, large metallic restorations (particularly without adequate insulation), or restorations with defective margins.
Acute Pulpits
Acute pulpitis usually occurs in a tooth structure with a large carious lesion or restoration, commonly a defective one around which there has been ‘recurrent caries.
Severe toothache is elicited by thermal changes on tooth structure, particularly those caused by ice or cold drinks. Characteristically, this toothache persists even after the thermal stimulus has disappeared or been removed. It increases sensitivity to both heat and cold of tooth structure.
The pulpal pain is poorly localized in tooth structure and may be felt in any of the teeth structure of the upper or lower jaw of the affected side, since the pulp of the individual the tooth are not represented precisely on the sensory cortex. As a greater proportion of the pulp becomes involved with intrapulpal abscess formation, the toothache may become even more severe and is often described as lancinating or throbbing type, The toothache generally lasts for 10-15 minutes but may be more or less continuous, and its intensity may be increased when the patient lies down. The application of heat may cause an acute exacerbation of toothache.

Chronic Pulpits
Toothache is not a prominent feature of chronic pulpitis, although sometimes the patient complains of a mild, dull ache in tooth structure, which is more often intermittent than continuous. The reaction to thermal change in tooth structure is dramatically reduced in comparison to that in acute pulpitis. Because of the degeneration of nerve tissue in the affected pulp, the threshold for stimulation by the electric pulp vitality tester is often increased, in contrast to cases of acute pulpitis, in which it is usually decreased.