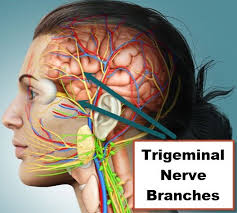
The trigeminal neuralgia is also called as Tic doulouroux, Trifacial neuralgia or Fothergill’s disease. Severe pain occuring along the course of nerve.
Etiology :
Based on etiology it is idiopathic or secondary.
Idiopathic Trigeminal Neuralgia :
Dental pathosis leads to involvement of trigeminal neuralgia.
Secondary to extensive traction on various divisions of fifth nerve being influenced by maxillo-mandible relationship.
It can be secondary to an allergic and hypersensitivity reaction causing oedema of trigeminal nerve root.
Secondary Trigeminal Neuralgia :
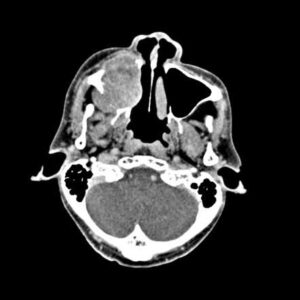
Conditions such as carcinoma of maxillary antrum, nasopharyngeal carcinoma and tumours of peripheral nerve root can cause secondary trigeminal neuralgia.
Benign tumours, as well as intra cranial vascular anomalies may present trigeminal pain.
Multiple sclerosis is usually associated with trigeminal neuralgia.
Clinical Features :
Age: It usually occurs in middle and old age, disease seldom occurs before 35 years of age.
Sex: Females are more commonly affected.
Site: It is most common in right side and lower portion of face is most commonly affected.
Nature of pain: Pain is paroxysmal, lasting only few seconds to few minutes and is of extreme intensity. It may be described by the patient as resembling to knife like stab lightning’ electric shock, stabbing or lancinating type of pain.
Aggravating factors: The pain is provoked by obvious stimuli to face. A touch or a draft of air, any movement of face as in talking, chewing yawning and swallowing may evoke lancinating attacks.
Trigger zones: These are the zones which precipitate an attack when touched. The trigger zones are vermilion border of lips, ala of nose, cheeks and around the eyes. The patient avoid touching the skin over trigger zones which makes him go unwashed or unshaven for many days.
The pain is confined to the trigeminal zone, nearly always unilateral and if bilateral is successive, rather than concomitant.
Management :
Elimination of all possible sources of infection.
Medical Treatment :
Trichloro ethylene inhalation is given.
Anti-cholinergic drugs are given.
Dilantin is given orally i.e., 300 to 400 mg per day. It is given in single or divided doses.
Carbemazepine (tegretol) has affect on paroxysmal pain. 100 mg is given twice a day untill relief is established.
Baclofen as anti spasmodic drug is also used.
Clonazepam which is an antiepileptic may also be used.
Anti-inflammatory agents like Indomethacin and short courses of steroids are useful.
Surgical Treatment :
Injection of nerve with anaesthetic solution is given in peripheral branches of trigeminal nerve serve as to provide temporary relief.
Injection of nerve with alcohol leads to neurolysis of affected nerve and patient get relief for 6 to 24 months.
Peripheral neurectomy i.e., nerve sectioning and nerve avulsion. This procedure is more lasting and affective than injection with alcohol.
Electrocoagulation of gassarian ganglion: Diathermy apparatus is placed in gasserian. ganglion to coagulate and destroy it.
Percutaneous radiofrequency trigeminal neurolysis: In this controlled radiofrequency is used/It is performed by insertion of temperature monitoring electrode through foramen ovale in trigeminal ganglion,
Rhizotomy: Actual cutting of trigeminal sensory root results in permanent anesthesia in more patients.